Can we learn anything from the experience of Malaysia and Indonesia?
Viral protease inhibitors

I have been following the Covid-19 pandemic in Malaysia as I have visited this country on several occasions. It is a good example of a country very close to the Equator, and by contrast the UK is closer to the North Pole than to the Equator.
Quiet in 2020
While the UK and Europe were experiencing large numbers of cases and deaths from Covid-19 during early and late 2020, all was quiet in Malaysia (population 32.7 million, see Figure 3) and neighbouring Indonesia (population 273.5 million), even though they are very close to China, the epicentre of the pandemic.
In the UK, the high numbers in early 2020 diminished as expected in the Spring and Summer, as a result of the production of vitamin D in our skin with the mid-day Sun being more than 45 degrees above the horizon. This gives the ambient sunlight a sufficiently high energy to break the specific intramolecular bond in the 7-dehydrocholesterol (7-DHC) molecule synthesised in the skin so as to form Vitamin D (see Figure 1).
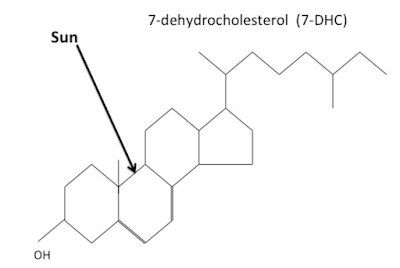 |
| Figure 1. Action of UV on the molecule of 7-dehydrocholesterol (7-DHC) |
Figure 2, below, shows how the pandemic in the UK settled during mid-2020, under the influence of Vitamin D produced in the skin.
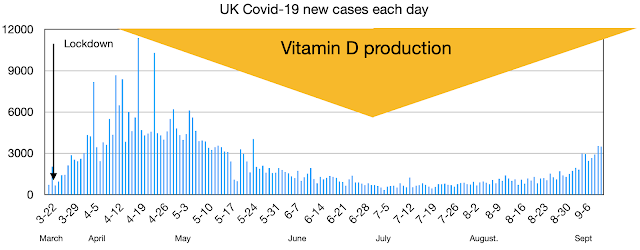 |
| Figure 2. UK: Covid-19 cases each during 2020 |
At the Equator, UV from the Sun has high intensity all the year round, giving those who live there the opportunity for adequate vitamin D production with subsequent optimal immunity and health advantages. This was the most obvious and most simple explanation for the low numbers and deaths from Covid-19 during the early part of 2020, despite the close proximity to China. However this did not continue and Covid-19 cases increased rapidly in late 2020. This must be regarded as the arrival of the virus, as there are no solar seasons close to the equator.
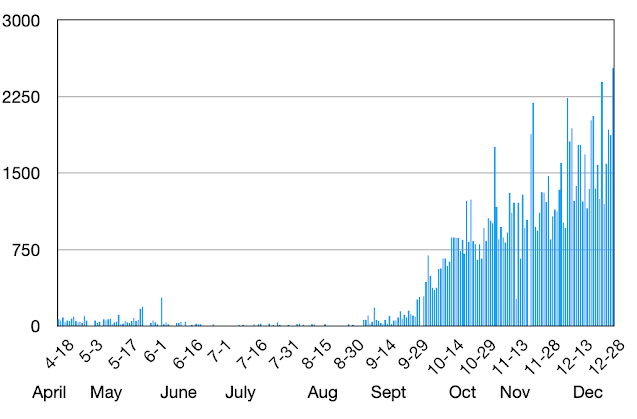 |
| Figure 3. Malaysia – Covid-19 cases per day 2020 |
Adjacent Indonesia (Figure 4) showed a similar pattern during 2020. In relationship to populations size, the cases in Malaysia were much higher than in Indonesia. The reason for this is not obvious.
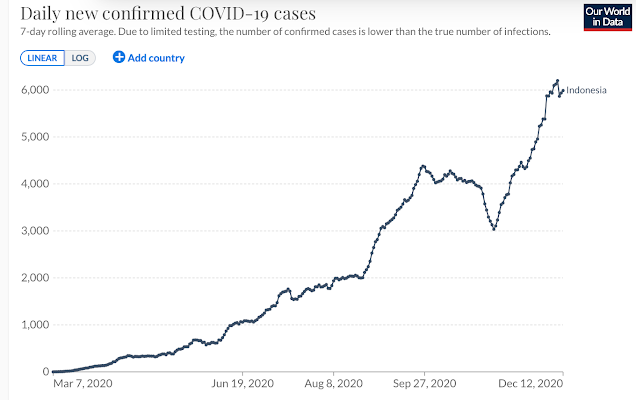 |
| Figure 4. Indonesia – Covid-19 cases per day 2020 |
Note in Figure 3 that in late 2020 there was a maximum of 2,250 cases per day in Malaysia. We can regard this as "quiet", especially if we display it in the same scale (Figure 5) that will be used for 2021 (Figure 6).
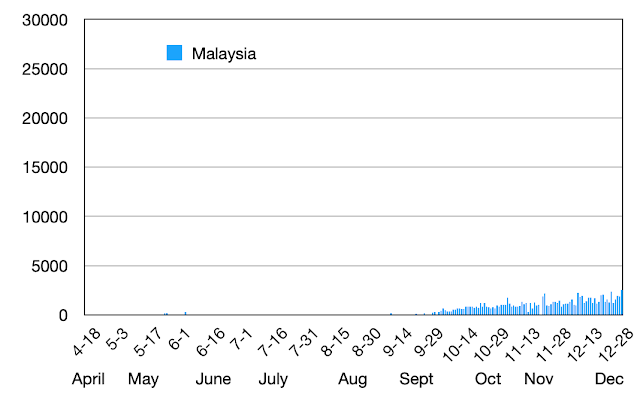 |
| Figure 5. Malaysia – Covid-19 cases per day 2020 (same data as Figure 3, but different scale) |
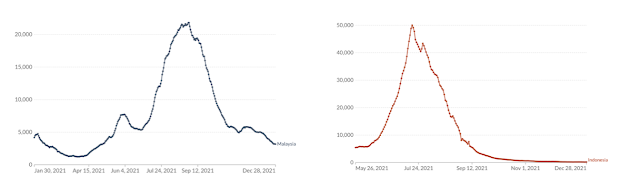
The early months on 2021 continued to be "quiet" in Malysia, Covid-19 case numbers reaching a maximum of about 5,000 per day. However during the latter part of the 2021 there was a considerable increase in cases to 22,500 per day (Figure 6).
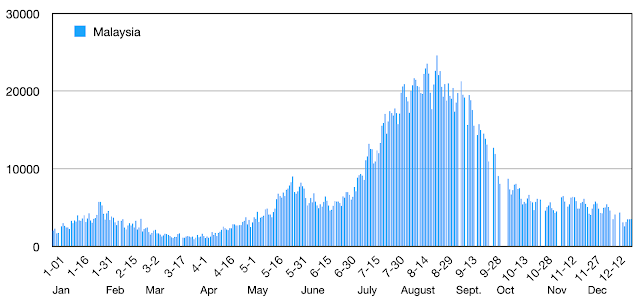 |
| Figure 6. Malaysia – Covid-19 cases each day in 2021 |
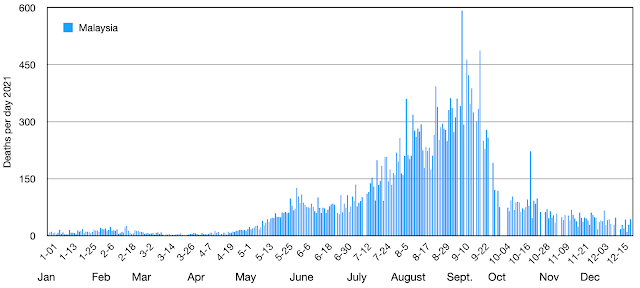 |
| Figure 7. Malaysia – Covid-19 deaths each day in 2021 |
The reason for this was not obvious. With Covid-19 cases being so low for more than year, why was there was such a dramatic increase in June 2021? What happened immediately before the increase that might have caused it?
The answer is a major vaccination programme, starting at the beginning of June 2021 (Figure 8).
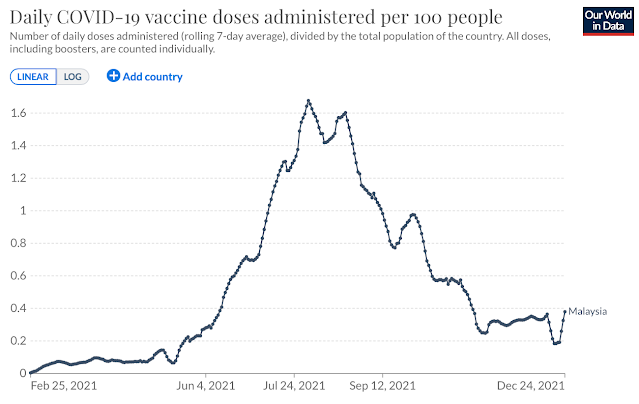 |
| Figure 8. Malaysia – vaccination initiative starting in early June 2021 |
The vaccination initiative was similar in Indonesia (Figure 9), but more gradual as the country is much larger and widespread than Malaysia.
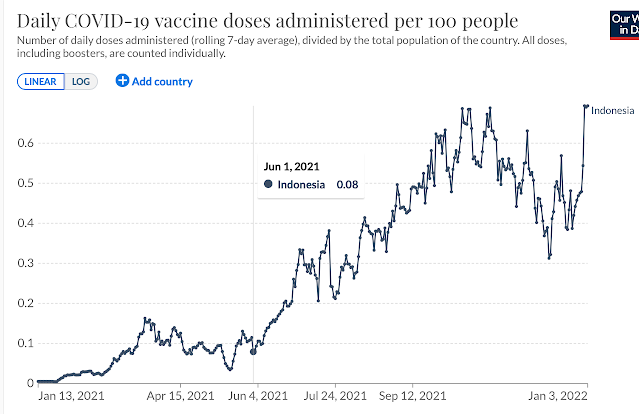 |
| Figure 9. Indonesia – vaccination initiative starting in early June 2021 |
We are seeing what also occurred in many if not most countries of the world, a large increase of Covid-19 immediately following the onset of a large vaccination initiative.
Reason for Covid-19 increase following vaccination initiative
Why might a vaccination programme cause such a surge in Covid-19 cases? Some people might regard it as a direct "poisoning" effect of the vaccines, with damage to immune mechanisms, but I suggest an alternative explanation which would be readily reversible. It all depends on the vitally important role of VItamin D, which appears to be understood by very few people, including our officials.
To recap: most of our Vitamin D is produced in the skin from synthesised 7-DHC. Otherwise it is taken by mouth, or it can be given by injection. However it all passes in the blood stream to the liver. Here it undergoes slow hydroxylation to form 25(OH)D, which is the important reserve circulating in the blood. It is also known as calcidiol or calcifediol. When required for immune escalation, this is taken into the immunity cells and further hydroxylated to its active form 1,25(OH)D, calcitriol.
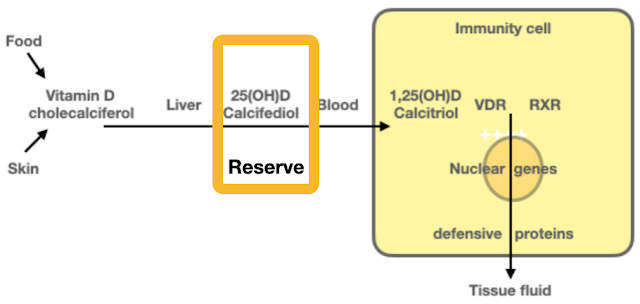 |
| Figure 19. Vitamin D and its essential role in defensive immunity |
I have discussed this in a recent Blog post. The vaccination induces an intense inflammatory immune reaction, which involves activation of T-cells and other cells of immunity. It requires the appropriate nuclear genes to be switched on, and for this the intracellular heterodimer VDR–RXR must be activated. And what is essential for the activation of VDR specifically? Vitamin D in its own fully activated form 1,25(OH)D, calcitriol.
We need a full tank
We never know when we are going to encounter a serious infection, such as Covid-19, but when we do it is essential to have a good reserve of vitamin D as 25(OH)D in the blood. This will be required to activate the defensive immune response.
It is like a car journey. If we are setting out on a long and uncertain car journey it is both sensible and indeed essential to have a full fuel tank. If not there is a danger of "conking out", coming to a halt in the middle of nowhere, or possible on a busy motorway.

And so it is with Vitamin D. If we encounter a serious infection and we have a low reserve of Vitamin D in the blood, there is a danger of critical illness or death. We can "conk out" in just the same way as the car with an empty tank. Unlike a car, we do not have Vitamin D level indicator, but these days it is simple to have the blood level of Vitamin D tested.
We know the critical blood levels of Vitamin D. Experience from Israel has confirmed previous experience that a blood level greater than 40ng/ml (100nmol/L) is safe, a full reserve. On the other hand a level of 20ng/ml (50nmol/L) is very low, and there is a risk of danger ahead.
Fuel, power, and Vitamin D comsumption
There is another analogy. When driving a car on a long journey it is essential to have a full tank because fuel can only be used once. When it has been used (combustion) all that remains is exhaust gases. There is a limit to the number of miles or kilometers to the gallon or litre, or to a full battery charge. When diesel, petrol or battery charge are consumed, the tank must be refuelled or the battery recharged.
Fuel/power consumption is low at steady state "Green" speeds, but it increases when the car is driven faster (fuel consumption is high at low speeds as inefficient low gears are used). In a similar way, Vitamin D comsumption is low when we are in steady state good health, but when we are ill, when disease is actve, Vitamin D consumption increases to enable defensive immunity.
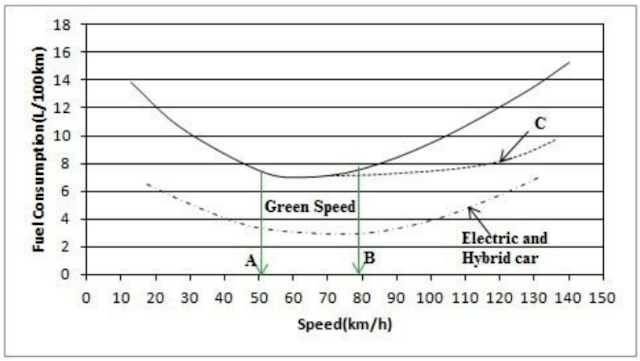 |
| Figure 20. Fuel consumption related to car speed |
A constant amount of Vitamin D as the circulating 25(OH)D is essential to supply its intracellular activated form 1,25(OH)D, which links to and activates VDR (Vitamin D Receptor). The VDR–RXR dimer switches on appropriate genes, but it also automatically stimulates the enzyme 24-hydroxylase. This is safety mechanism that converts 1,25(OH)D into 24,25(OH)D. This is an irreversible process and 24,25(OH)D is inactive. a molecule of vitamin D can only be used once.
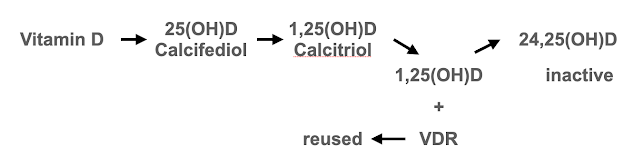 |
Figure 21. Vitamin D molecule can only be used once |
This a success of evolution. If 1,25(OH)D were to remain active, then during an immune escalation the level of 1,25(OH)D would build up to toxic levels. The enzyme 24-hydroxylase ensures that this does not happen. However it necessitates a constant supply of vitamin from the skin or by mouth, and a large reserve of 25(OH)D in the blood to iron out as much a possible natural fluctuations of Vitamin D production during the year.
Vitamin D deficiency in Malaysia and Indonesia
It might be thought that people living in Malaysia and Indonesia, both on the equator, have good reserves of Vitamin D with all year round production of it. But not so. 90% of babies born in Indonesia are deficient of Vitamin D, and this represents the Vitamin D status of their mothers. During childhood Vitamin D levels increase as a consequence of exposure to the Sun. but this is constrained in adult life.
Generally people in hot tropical countries avoid the Sun as much as possible. . But it is important to remember that Malaysia and in particular Indonesia have very large Muslim populations, and skin cover by clothing is carried to extremes. UV from the Sun does not penetrate most clothing, and so Vitamin D deficiency is inevitable.
Vitamin D deficiency and Covid-19 vaccination
How many of the populations of Malaysia and Indonesia develop mild or subclinical Covid-19 during 2020 is unknown, but they must have encountered the vaccination programme when generally deficient of Vitamin D. The intense immune response following vaccination (and it definitely is intense as judged by the high frequency of mild and transient symptoms) will have consumed a great deal of Vitamin D, but the quantity involved is unknown. As far as I am aware there has been no research so far on the effect of vaccination of blood levels of Vitamin D.
Figure 22 illustrates what will be happening. Vitamin D will be sunsumed by vaccinations, and at this time of the year without natural replenishment. The blood level of Vitamin D will inevitably go down and might reach critically low levels – unless a Vitamin D supplement is taken (dose about 4,000 units daily).
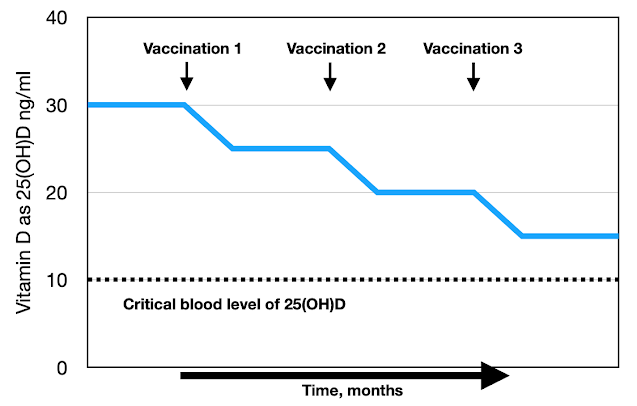 |
| Figure 22. Illustration of the effect of vacc=inations on VItamin D |
The mass vaccinations must have resulted in mass serious and critical Vitamin D deficiency. The immune process cannot happen without consuming Vitamin D. In fact without adequate Vitamin D the vaccinations could not have given the expected level of protection against Covid-19 – the level and duration of protection has been much less than anticipated, hence so many cases among the vaccinated.
Viral protease inhibitors
The peaks obviously settled, as they always do. But here we see a difference between Malaysia and Indonesia.
In Malaysia the decline of cases and deaths dropped but not completely. There is a continuing steady state of 3,000 to 4,000 cases per day, and 20 to 40 deaths per day.
On the other hand in Indonesia there are many fewer at 100 to 200 new cases each day and only about 10 deaths each day.
 |
| Figure 23. Malaysia & Indonesia Covid-19 cases per day – the endings of the peaks |
This difference is interesting. I can think of only one plausible answer and that is the additional therapeutic intervention in Indonesia. I am not aware of Vitamin D supplements being given to the population, but apparently Ivermectin therapy was adopted in Indonesia on September 1st 2021. This went against the advice of the WHO, but it was based on the experience of several countries in the east which had good results from Ivermectin, together with much published evidence.
Ivermectin
I have not followed the Ivermectin story in detail and I am by no means an expert on it. It appears that Ivermectin is "controversial" and it seems to be clear that there has been a successful and co-ordinated mis-information campaign against it. A meta-analysis of 74 papers evaluating Ivermectin showed benefit in 71 of them. I suspect that most informed people accept the value and safety of Ivermectin within its recommended dose, but very few people are informed. This has been the problem during the Covid-19 pandemic: we have not been supplied with much information, just sound-bites.
The most absurd and desperate reason to be vaccinated against Covid-19 came from the UK Prime Minister Boris Johnson as reported in the national press on Christmas Eve:

Among other properties, Ivermectin is a viral protease inhibitor, which makes it effective against a number of mammalian parasites, including viruses.
Pfizer has developed its own viral protease inhibitor, during development known as PF-07321332, and unofficially as "Pfizermectin". On December 23rd 2021 it received an Emergency Use Authorisation (EUA) from the US FDA. It is now called Paxlovid.
Now we see why Ivermectin has been ridiculed and buried. Patients with Covid-19 have been told officially that there is no treatment available. They have been denied treatment with Ivermectin 12mg per day for five days from the onset of symptoms. 30 years experience has shown an excellent safety profile of Ivermectin in the correct dose.
The EUA for Paxlovid was given on the "understanding" that there were no other treatments available for Covid-19, hence the essential denial and burial of Ivermectin.
Exactly the same thing happened with Vitamin D, official denial that it might be of any benefit so that EUAs could be granted for the vaccines.
The main problem with both Vitamin D and Ivermectin is that they are too cheap. There is no big money to be made, unlike with vaccines and Paxlovid, which will be sold at several hundred times the price of Vitamin D and Ivermectin.
Perhaps it is true to say that the Covid-19 pandemic has been an exercise in transfering money from the poor (the great majority of us) to the very rich. In the process there have been many avoidable deaths and undue pressure being put on the hospitals.
Vitamin D consumption
But the most important thing at present is the rapid escalation of cases, especially on North America and Europe. My interpretation is that the undoubted intense inflammatory immune response to the vaccinations is inevitably consuming Vitamin D (Figure 22). The resulting immune deficiency is driving the increase in cases, which although usually mild will consume even more Vitamin D, and so we can expect infections of all sorts to become more frequent. This is particularly important during the winter months as it will be a few months before we start to produce Vitamin D.
New York has experienced a cluster of tuberculosis. This infection is well-established as developing when immunity is suppressed, as in AIDS, but also resulting from Vitamin D deficiency.
There is every medical reason why Vitamin D should be used extensively at the present time, especially if vaccinations are being given increasingly and at shorter intervals.
Vitamin D is needed now.
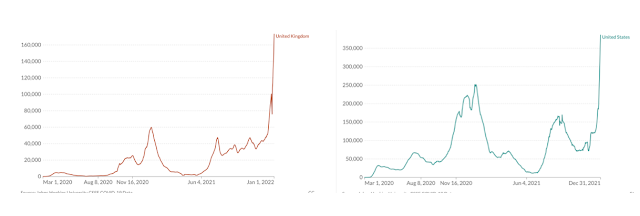 |
| Figure 24: Covid-19 cases per day UK & USA at the end of 2021 |