At
one time life was simple and we knew all the answers. The cause of disease (and
everything else) was God, often acting in response to the sins of mankind. The
public health officials of the time might have advised “less sin”, but either
the population ignored the advice or the concept was flawed.
The
most important discovery of the Age of Enlightenment was “ignorance”, the
realisation that divine intervention was at the very best unreliable, and
probably non-existent. We were therefore ignorant of the causes of disease.
Yuval
Noah Harari, in his remarkable book “Sapiens - a brief history of humankind”
proposes that the unique attribute of Homo
sapiens, the present humankind, is our ability to create abstract ideas,
to create fictions. Our many gods are clear examples of this. Fictions are our
attempt to explain the world as we experience it. We use fictions to try to make
sense of the diseases that afflict us. Often these indicate the blaming of the
victims for the errors of their ways, eating the wrong foods, not taking
sufficient exercise, or, the greatest sin of all, smoking.
In
the absence of divine activity we must search for physical explanations for
diseases. We can classify inherited disorders, which can be genetic (from the
moment of conception) and congenital (abnormalities of our construction), and
both of these in the past have been ascribed to divine retribution for the sins
of the parents. Disease acquired after birth can be due to environmental
factors, which can be physical (injury, heat, cold), chemical (poisons meaning
too much, or deficiencies meaning too little), or biological (a wide variety of
micro-organisms).
The
elusive nature of “proof” is described and advanced by “Hill’s Criteria”, in an
associated Post.
Science
starts with observation. We look for clues to give us a way to construct a
fiction of causation, called a theory or hypothesis, or a paradigm when it
receives general acceptance. But fictions are not absolute truths and fictions
change with increasing knowledge.
Causation
is complex. For example we have seen that although we accept that cigarettesmoking is the major cause of lung cancer, the fact that only 10% of
heavy smokers die from lung cancer indicates that other factors must be
considered. These can be viewed as “susceptibility factors”, or perhaps
“protective factors”. We can regard disease as the result of interaction
between “the cause” together with susceptibility or protective factors, which
might be genetic or environmental.
Clues
to the identification of susceptibility and protective factors, and indirectly
to causation, can be gained from comparing disease incidence in different
populations, that is the geography of disease. This is an important dimension
of epidemiology. An example is the “Greek paradox”.
I
have been warned that data from Greece may not be entirely reliable as it is a
country with an unusually well-developed culture of fiction. However WHO data
that includes Greece is the best data that we have and we cannot ignore it.
Greece
apparently has the highest prevalence of cigarette smoking in Western Europe,
as we can see in Table 1. (cigarette smoking has a higher prevalence in the
former Soviet countries in Eastern Europe)
 |
| Figure 1: percentage of adults who smoke |
However
Greece has within Europe the lowest age-standardised death rate from coronary
heart disease (CHD). The paradox is that cigarette smoking is considered to be
a major causative factor of CHD. Where there is a high prevalence of cigarette
smoking we expect to find a high death rate from CHD, but not so in Greece. In
Table 2 we see age adjusted death rates in men from myocardial infarction (data
from WHO 1986).
 |
| Figure 2: age standardised death rates from myocardial infarction |
Why
is it that cigarette smoking in Greece
does not cause the high incidence of premature death from CHD that it does in
other countries?
“The Seven Countries Study” written Ancel Keys has
been the subject of a previous Post. Although methodology was far from perfect
and conclusions were not very objective, the study provides a great deal of
data. It was very influential in its false conclusion that animal fats cause CHD,
and this led to inappropriate diet manipulation over a period of 50 years,
continuing to present time.
The
study recorded CHD death rates in population samples in some countries within
western and central Europe. From the data presented we are able to see that as
expected the risk of a man dying from CHD increases with the number of
cigarettes smoked. This is obvious if we look at countries in Northern Europe.
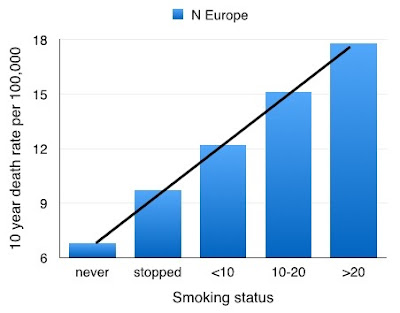 |
| Figure 3: CHD death rates and smoking - northern Europe |
The slope of the graph-line rises steeply, indicating that as the number of
cigarettes smoked increases, the CHD death rate increases substantially.
However
the slope of the graph-line is different in what was then Yugoslavia, mainly
Serbia (study population from Belgrade). In this more central country of
Europe, the graph-line once again shows an increasing incidence of CHD death
with an increasing number of cigarettes smoked, but the graph-line is not as
steep.
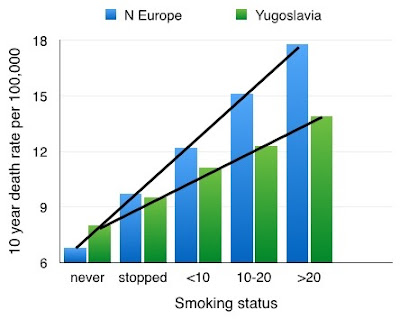 |
| Figure 4: CHD death rates - northern and central Europe |
This
indicates that the damaging effects of smoking in Serbia are not as great as in
the northern countries.
If
we now look at Greece and Italy, countries in the south of Europe we see a graph-line
that is almost flat.
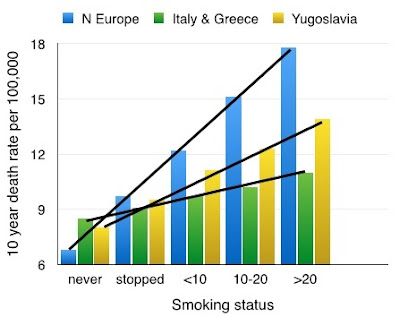 |
| Figure 5: CHD death rates and smoking in Europe |
This
indicates that the risk of CHD death at the age in the study is very low in
those who do not smoke, and this is what we expect. However the risk increases
only marginally in those who smoke heavily.
What
this means is that the risk of a heavy smoker dying from CHD increases
dramatically as we move north through Europe. If we look at the low or no
cigarette smoking rates in the three European regions we see little difference.
If however we look at the heavy smoking group we see a major difference.
It
appears to be fairly safe someone in Greece to smoke heavily but it is very
dangerous for someone in the northern countries of Europe.
But
this feature of Greece and Southern European countries is seen in more diseases
than CHD. There is a similar observation of the incidence of breast cancer and
colon cancer having a diminishing incidence in the south of Europe compared to
the north.
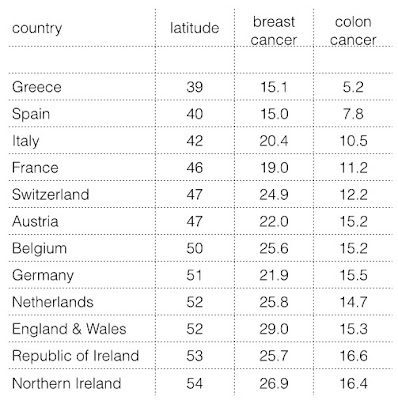 |
| Figure 6: cancer rates and latitude in Europe |
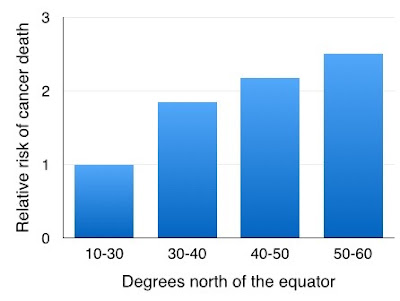
The
first observation of a latitude effect of cancer incidence was in North
America.
 |
| Figure 7: Cancer and latitude in Americas |
Death
rates from cancer increase in the northern parts compared to the southern
parts.
The
obvious and most simple difference between places closer compared to more
distant from the equator is the climate, and in particular the different
intensity of the sun.
The observations of cancer death rates and the
effect of cigarette smoking on CHD death supports the proposal that exposure to
the sun (avoiding severe sunburn) is a great advantage to our health, and
reduces the risk of damage from cigarettes.
There
is evidence of a help from vitamin D and the sun in thosewho are diagnosed with
lung cancer, in an associated Post.
If someone wishes to enjoy good health and a
long life but nevertheless wishes to smoke, then it is advisable
to live in Greece - see Post Sir Patrick Leigh Fermor (died aged 93).





























